"Abstract
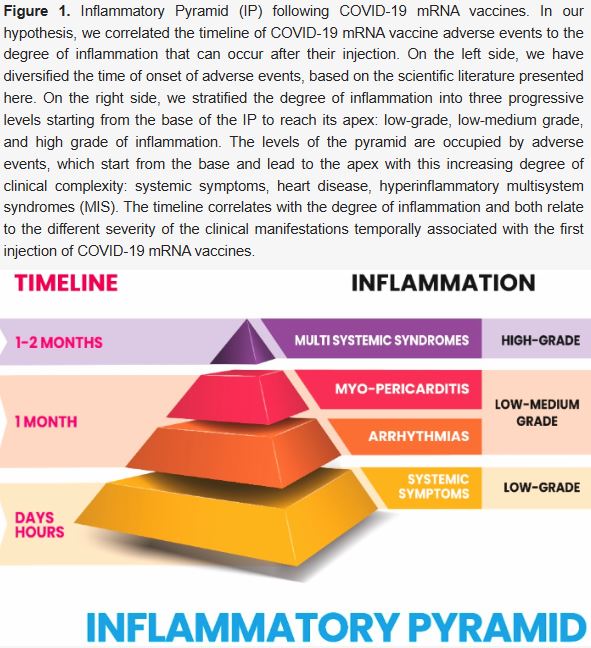
Each injection of any known vaccine results in a strong expression of pro-inflammatory cytokines. This is the result of the innate immune system activation, without which no adaptive response to the injection of vaccines is possible. Unfortunately, the degree of inflammation produced by COVID-19 mRNA vaccines is variable, probably depending on genetic background and previous immune experiences, which through epigenetic modifications could have made the innate immune system of each individual tolerant or reactive to subsequent immune stimulations. We hypothesize that we can move from a limited pro-inflammatory condition to conditions of increasing expression of pro-inflammatory cytokines that can culminate in multisystem hyperinflammatory syndromes following COVID-19 mRNA vaccines (MIS-V). We have graphically represented this idea in a hypothetical inflammatory pyramid (IP) and we have correlated the time factor to the degree of inflammation produced after the injection of vaccines. Furthermore, we have placed the clinical manifestations within this hypothetical IP, correlating them to the degree of inflammation produced. Surprisingly, excluding the possible presence of an early MIS-V, the time factor and the complexity of clinical manifestations are correlated to the increasing degree of inflammation: symptoms, heart disease and syndromes (MIS-V)...
10. Discussion
The injection of COVID-19 mRNA vaccines results in a strong expression and secretion of pro-inflammatory cytokines associated with a wide and variable cellular activation, both immune and vascular. In relation to the degree of inflammation produced by each subject, depending on its genetic status and the acquired condition of epigenetic modification of the innate immune system, systemic symptoms, heart disease, and hyperinflammatory syndromes can be produced as AEs.
In Table 2, some effects determined by the injection of COVID-19 mRNA vaccines are listed.
Different levels of expression of pro-inflammatory cytokines over time, after a COVID-19 mRNA vaccination, the persistence of the Spike protein in circulation for a prolonged period of time, the prolonged immune and inflammatory response against the Spike protein, the strong pro-inflammatory activity of LNP, the actions of the Spike protein on the Angiotensin II/AT1 axis, the activation of TLR4 and the TLR4/NFκB axis in cardiomyocytes by the Spike protein, and the endothelial dysfunctions produced by the Spike protein all together represent a series of subsets that can contribute with variable expression, especially to the pathogenesis of myocarditis and multisystem syndromes.
Biochemical studies revealed that Spike protein triggers inflammation via activation of the NF-κB pathway and the induction of pro-inflammatory cytokines, such as IL-6, TNF-α, and IL-1β. Furthermore, the expression of cytokines and chemokines, in response to Spike protein, was dose-dependent and this agrees with the different timeline of myo-pericarditis following COVID-19 mRNA vaccines (onset after second dose of BNT162b2 vaccine or at first and second dose of mRNA-1273 vaccine). After the first dose of the BNT162b2 vaccine, the human organism produces systemic inflammation which is accompanied by the upregulation of TNF-α and IL-6 after the second dose.
Furthermore, the S1 subunit of the Spike protein produces an endothelial lesion that is amplified by simultaneous exposure to the inflammatory cytokine TNF-α and the male hormone dihydrotestosterone."
© 2023 by the authors. Licensee MDPI, Basel, Switzerland.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).